Fatty liver doesn’t stop gallbladder surgery, but it changes the game plan. Surgeons take extra care to reduce bleeding and protect liver function during cholecystectomy. Recovery may need tighter diet control, liver-friendly medications, and closer follow-up. Bottom line: outcomes are good—but precision, planning, and post-op discipline matter more.
Under the experienced care of Dr Ashutosh Nayak, outcomes remain predictable and controlled. This guide explains what actually changes, what stays the same, and why early action matters if you plan Laparoscopic gallbladder surgery in kolkata.
Does fatty liver stop you from having gallbladder surgery?
No—fatty liver usually doesn’t prevent gallbladder surgery. It simply requires careful surgical planning and closer monitoring to ensure a safe outcome. Risk depends on severity, liver function, and metabolic health. Surgeons modify evaluation and intraoperative strategy.
Most people with mild fatty liver can still have laparoscopic surgery
Most patients with mild (Grade 1–2) fatty liver can safely undergo gallbladder surgery in fatty liver without delay. With stable labs and proper evaluation, outcomes and recovery are usually similar to standard cases—while delaying care increases risk.
The plan changes more when fatty liver is advanced (fibrosis/cirrhosis concerns)
When fatty liver progresses to fibrosis or cirrhosis, surgical planning becomes more cautious and individualised.
Surgeons assess –
- Bleeding risk
- Signs of portal hypertension
- And anaesthesia tolerance
Some patients need hepatology clearance. This reflects careful NAFLD gallbladder surgery precautions, not denial of surgery. Advanced liver disease shifts timing, not intention. Surgeons prioritise stabilisation first. Then they proceed with a controlled laparoscopic approach when safe.
Fatty liver in simple terms (and why it often shows up with gallstones)
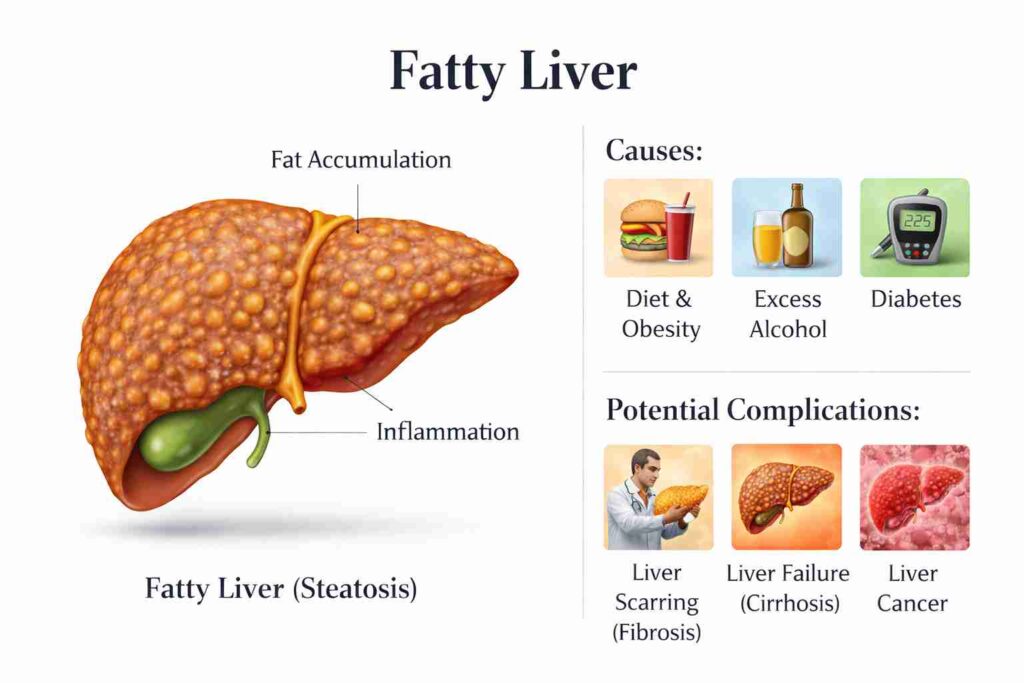
Fatty liver is the buildup of excess fat in the liver, often driven by insulin resistance and poor metabolism. The same imbalance thickens bile and slows gallbladder emptying—making gallstones and fatty liver show up as a common duo.
NAFLD/MAFLD basics: fat in the liver, often linked with weight/diabetes
Non-Alcoholic Fatty Liver Disease (NAFLD) is now increasingly termed Metabolic Dysfunction-Associated Fatty Liver Disease (MAFLD) or Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD). It is the most common chronic liver disease worldwide
and affects nearly 25% of adults. [Source].
It stems from metabolic overload. Sugar, sedentary behaviour, and visceral fat accelerate visceral fat accumulation. Symptoms rarely appear early.
When physicians detect the condition early, patients can undergo appropriate evaluation and proceed with gallbladder surgery with fatty liver safely.
Why do gallstones and fatty liver commonly travel together
Fatty liver and gallstones share the same root—insulin resistance that thickens bile and slows gallbladder emptying.
That’s why they often appear together, making a combined approach to fatty liver and gallstones treatment essential for lasting results.
| Shared Factor | Effect on Liver | Effect on the Gallbladder |
| Insulin resistance | Fat storage | Cholesterol supersaturation |
| Obesity | Inflammation | Reduced gallbladder emptying |
| High sugar intake | Triglyceride buildup | Stone formation |
What changes before surgery (pre-op evaluation)
Preoperative testing becomes more focused when fatty liver exists. Surgeons assess liver function, coagulation status, and anaesthesia safety. Early correction prevents bleeding and delayed recovery.
Which tests matter: LFTs (SGPT/SGOT), ultrasound notes, platelet count
Doctors examine trends in enzyme levels, not single values. Mild elevation rarely stops surgery. Persistent rise demands review. This addresses concerns regarding high SGPT SGOT gallbladder surgery planning.
Key LFTs (Liver Function Tests) include:
- Liver function profile
- SGPT (ALT): Serum Glutamate Pyruvate Transaminase
- SGOT (AST): Serum Glutamate Oxaloacetate Transaminase.
- Platelet count
- Ultrasound liver texture
- Blood sugar control
When the surgeon may ask for fibrosis assessment or specialist clearance
Surgeons may request fibrosis assessment or specialist clearance when labs or imaging suggest advanced liver disease. This helps evaluate the laparoscopic cholecystectomy fatty liver risk and ensures the procedure is planned with maximum safety.
Medication and anaesthesia planning considerations
Medication and anaesthesia are carefully tailored to protect liver function and avoid added stress during surgery. This helps minimise the risk of fatty liver anaesthesia for surgery and ensures a smoother, safer recovery.
What changes during surgery (what surgeons mean by “a difficult gallbladder”)
During surgery, a “difficult gallbladder” refers to inflammation, scarring, or fatty changes that distort normal anatomy and increase the risk of bleeding. This demands slower, more precise dissection and experienced surgical judgment to ensure safety.
A fatty/enlarged liver can make exposure harder (retraction and visibility)
A fatty or enlarged liver can limit visibility and make retraction more challenging during gallbladder surgery in a fatty liver. This reduces working space, requiring careful handling and precise technique to maintain a clear, safe operative field.
Bleeding risk: why the liver bed can ooze more
Bleeding risk is higher because a fatty liver is more fragile and its blood vessels don’t seal as cleanly. The liver bed may ooze more during dissection, requiring meticulous control to keep the field safe and clear.
Longer operative time or conversion to open: when it’s considered (safety-first)
A longer surgery does not necessarily indicate that something went wrong. Surgeons may convert to an open approach if visibility or anatomy becomes unsafe. That decision prioritises patient safety, not speed.
This remains rare in experienced hands like Dr Ashutosh Nayak, performing laparoscopic cholecystectomy in Kolkata.
When a drain might be used and why
A drain prevents fluid buildup after a difficult dissection. Surgeons may place a drain after a difficult dissection to monitor fluid or bleeding. It offers early warning, not bad news. Doctors remove it quickly once recovery looks stable.
| Surgical Challenge | Why It Happens | Surgeon Response |
| Enlarged liver | Fat infiltration | Modified retraction |
| Oozing surface | Fragile tissue | Energy sealing |
| Dense adhesions | Chronic inflammation | Slow layered dissection |
What does NOT change (important reassurance)
The surgical goal stays identical. Surgeons remove the gallbladder safely. Laparoscopy remains the standard method. Recovery protocols largely match routine cases.
The goal: remove the gallbladder safely (laparoscopic is still standard in most cases)
The goal is simple—safe and complete gallbladder removal surgery, with a laparoscopic approach remaining the standard in most cases. Even with added complexity, precision and technique ensure effective outcomes with faster recovery.
Most recovery instructions remain similar
Patients walk early. They eat light meals. They resume activity gradually. Dr Ashutosh Nayak mirrors standard protocols for laparoscopic gallbladder surgery in kolkata.
Risks and “red flags” after surgery (especially relevant if liver health is poor)
Early warning signs are more important when liver reserve remains reduced. Prompt reporting prevents escalation. Most patients recover without incident.
Monitor for fever, worsening abdominal pain, jaundice, persistent vomiting, or swelling. These signs may suggest infection, bile leak, or liver stress. Immediate reporting enables timely intervention and prevents escalation.
When to seek urgent care: fever, worsening belly pain, jaundice, persistent vomiting
These symptoms may signal infection or bile leakage. Immediate evaluation protects recovery, prevents escalation, and directly influences outcomes among vulnerable patients.
Expected vs abnormal post-op liver enzyme changes (high-level explanation)
A brief rise in enzyme levels after surgery remains common and usually resolves quickly. Persistent elevation suggests liver stress or obstruction and demands review, especially during high SGPT and SGOT gallbladder surgery follow-up.
Diet and recovery: the two-track plan (post-cholecystectomy + fatty liver improvement)
Recovery follows two parallel tracks. Patients must support digestion after gallbladder removal while correcting the metabolic drivers of fatty liver. Structured eating, gradual activity, and weight control protect healing and improve long-term liver health.
Short-term after gallbladder removal: low-fat, smaller meals, gradual normalisation
Early weeks require gentle digestion. Small meals reduce diarrhoea risk. Gradual normalisation and reintroduction of dietary fat support healing after treatment for fatty liver and gallstones.
Long-term fatty liver reversal: weight loss targets, activity, sugar/alcohol reality check
Sustainable weight loss reverses disease. Daily walking improves insulin response. Sugar restriction matters more than fat avoidance.
This reduces any future laparoscopic cholecystectomy fatty liver risks.
| Recovery Phase | Diet Focus | Lifestyle Action |
| Weeks 1 to 3 | Low-fat meals | Gentle walking |
| Months 1 to 3 | Balanced intake | Structured exercise |
| Long term | Sugar control | Weight maintenance |
Does gallbladder removal worsen fatty liver? What studies suggest
Current research shows no proof that gallbladder removal directly worsens fatty liver. Liver progression is more strongly associated with obesity and insulin resistance.
Surgery treats gallstones. Metabolic health determines long-term liver outcome.
Association vs causation (what research shows and what it doesn’t prove)
Studies link obesity and insulin resistance with both conditions. Removal alone does not damage the liver. This supports informed decision-making for gallbladder surgery in patients with fatty liver.
Why metabolic risk factors (obesity/insulin resistance) matter more than the surgery alone
Long-term liver health depends on weight control and insulin balance, not the operation itself. Untreated metabolic disease drives the progression of fatty liver. Gallbladder surgery does not damage the liver. Good metabolic control protects recovery and future liver function.
This clarifies fears around fatty liver anaesthesia risk for surgery myths.
Choosing gallbladder surgery care in Kolkata (what to ask)
Hospital selection influences safety in patients with liver disease. Structured teams reduce complication risk. Experience shortens recovery.
Questions to ask: surgeon experience, laparoscopy facilities, anaesthesia team, ICU backup
These define quality during laparoscopic gallbladder surgery in kolkata.
Patients should ask direct questions:
- Surgeon case volume
- Advanced laparoscopy setup
- Liver-aware anaesthesia protocols
- Emergency support availability
What affects cost in Kolkata (hospital category, complexity, imaging, comorbidities)
Cost varies with hospital tier and liver complexity. Imaging, ICU backup, and disease severity influence laparoscopic gallbladder surgery cost in Kolkata.
When to consider a higher-level centre (suspected advanced liver disease)
Patients with cirrhosis need tertiary support. Specialised care improves survival and outcomes for laparoscopic cholecystectomy in Kolkata.
Let’s recap
Gallstones and fatty liver frequently coexist, but surgery is rarely impossible. Surgeons adjust evaluation, bleeding control, and anaesthesia planning.
Most patients still recover normally after Laparoscopic gallbladder surgery in kolkata when metabolic risks are addressed early. Delay invites inflammation and complications.
Early action from Dr Ashutosh Nayak helps protect both organs, shortens recovery, and prevents long-term liver damage. Structured diet, weight control, and follow-up remain essential after surgery.
Book a session to gain more clarity.
People Also Ask
Can I undergo a laparoscopic cholecystectomy if I have a grade 1/2 fatty liver?
Yes. Most patients with mild fatty liver disease safely undergo surgery after routine evaluation.
Are high SGPT/SGOT levels a reason to delay surgery?
Mild elevation rarely delays surgery. Surgeons interpret trends, not isolated values.
What foods should I avoid after gallbladder removal if I also have fatty liver?
Avoid excess sugar, fried foods, and alcohol. Focus on small, balanced meals.
How long does recovery take after laparoscopic gallbladder surgery?
Most patients return to light work in 1 week and to full activity within 3 weeks.